Seems like the ability to cash in your chips under a certain set of criteria defined when you have the cognitive ability would help.Staying healthy longer can mean more of us facing Alzheimer's which I see as becoming a more prevalent and expensive problem in the years ahead.
So you save money in the short run by staying healthy only to run up huge costs in the final years of a long life.
Seems like we cannot win.

Colleges
- AAC
- ACC
- Big 12
- Big East
- Big Ten
- Pac-12
- SEC
- Atlantic 10
- Conference USA
- Independents
- Junior College
- Mountain West
- Sun Belt
- MAC
- More
- Navy
- UAB
- Tulsa
- UTSA
- Charlotte
- Florida Atlantic
- Temple
- Rice
- East Carolina
- USF
- SMU
- North Texas
- Tulane
- Memphis
- Miami
- Louisville
- Virginia
- Syracuse
- Wake Forest
- Duke
- Boston College
- Virginia Tech
- Georgia Tech
- Pittsburgh
- North Carolina
- North Carolina State
- Clemson
- Florida State
- Cincinnati
- BYU
- Houston
- Iowa State
- Kansas State
- Kansas
- Texas
- Oklahoma State
- TCU
- Texas Tech
- Baylor
- Oklahoma
- UCF
- West Virginia
- Wisconsin
- Penn State
- Ohio State
- Purdue
- Minnesota
- Iowa
- Nebraska
- Illinois
- Indiana
- Rutgers
- Michigan State
- Maryland
- Michigan
- Northwestern
- Arizona State
- Oregon State
- UCLA
- Colorado
- Stanford
- Oregon
- Arizona
- California
- Washington
- USC
- Utah
- Washington State
- Texas A&M
- Auburn
- Mississippi State
- Kentucky
- South Carolina
- Arkansas
- Florida
- Missouri
- Ole Miss
- Alabama
- LSU
- Georgia
- Vanderbilt
- Tennessee
- Louisiana Tech
- New Mexico State
- Middle Tennessee
- Western Kentucky
- UTEP
- Florida International University
High School
- West
- Midwest
- Northeast
- Southeast
- Other
- Alaska
- Arizona
- California
- Colorado
- Nevada
- New Mexico
- Northern California
- Oregon
- Southern California Preps
- Washington
- Edgy Tim
- Indiana
- Kansas
- Nebraska
- Iowa
- Michigan
- Minnesota
- Missouri
- Oklahoma Varsity
- Texas Basketball
- Texas
- Wisconsin
- Delaware
- Maryland
- New Jersey Basketball
- New Jersey
- New York City Basketball
- Ohio
- Pennsylvania
- Greater Cincinnati
- Virginia
- West Virginia Preps
ADVERTISEMENT
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Union support
- Thread starter Marvin the Martian
- Start date
Or the opposite. God forbid you run up huge financial costs when you're young. Then you can be totally screwed later in life. Many of these policies have a lifetime cap on what they pay out and if you exhaust it early you're toast. I know a guy who was taking heavy doses of prednisone for years. For some that can turn your tissue into kleenex. He had an endoscopy done and it punctured a hole in his esophagus. He was in the hospital for almost 9 months. The hospital/doctors exceeded his health insurance lifetime cap. Now he's basically uninsurable.Staying healthy longer can mean more of us facing Alzheimer's which I see as becoming a more prevalent and expensive problem in the years ahead.
So you save money in the short run by staying healthy only to run up huge costs in the final years of a long life.
Seems like we cannot win.
A major incremental factor is health care providers.
This appears to be a legitimate concern shared by the medical community.
Meanwhile, medical schools have long limited enrollment to keep the supply of doctors low for financial reasons.
This is not true. Medical school enrollment has increased 50%+ since the early aughts.
Also note the following from that article:
"Congress limits the number of residency training slots because of a 1997 law that limits which programs receive funding through Medicare."
So it seems the number of trainees is increasing...there are just limited locations for them to take up residency. There have been bi-partisan bills proposed to change the residency cap legislation from 1997. I'm not sure what progress has been made to pass those bills.
Everyone is right, Healthcare is a giant cluster ****.
I always come back to believing in the checks and balances between the public and private sector in general as that to me is a good starting point.
When you look at other models globally they tend to work together (I think only two countries are 100% single payer).
More importantly I can point to other industries that have a competitive private and public balance like the post office, our school system or security.
Back in the day the fastest choice you had was two day service from the post office. Then a private company called fed ex said it will cost you more but we will deliver it if you absolutely, positively need to get it there overnight. That put pressure on the USPS.
That relationship has always been the public sector kept things affordable while the private sector made sure the government program kept up and offered a competitive product.
When you take one of those two away, in general the private sector gets greedy or the public sector gets complacent.
So in my head at a 50,000 feet level I think we need both to work together and compete against each other....which again is why I like Pete's vision of health care reform.
I always come back to believing in the checks and balances between the public and private sector in general as that to me is a good starting point.
When you look at other models globally they tend to work together (I think only two countries are 100% single payer).
More importantly I can point to other industries that have a competitive private and public balance like the post office, our school system or security.
Back in the day the fastest choice you had was two day service from the post office. Then a private company called fed ex said it will cost you more but we will deliver it if you absolutely, positively need to get it there overnight. That put pressure on the USPS.
That relationship has always been the public sector kept things affordable while the private sector made sure the government program kept up and offered a competitive product.
When you take one of those two away, in general the private sector gets greedy or the public sector gets complacent.
So in my head at a 50,000 feet level I think we need both to work together and compete against each other....which again is why I like Pete's vision of health care reform.
That's right, healthcare is nothing but weeds . . . and no one knows what the weeds are when they need medical services. They just know something's wrong and they need some help getting it taken care of.. . . healthcare is nothing but the weeds.
The weeds is how providers - and insurers - make their money. The weeds is the opaqueness in the health care system.
If you go in for a lacerated arm from a home DIY project, you just want it fixed, and if you ask "how much" you're only impeding getting the arm fixed. If you ask "how much" and they say "$1500 to stitch you up" they don't mention the extra charges for the anesthesia, hypodermic needle for the anesthesia, disinfectant, coagulants, stitch material, the needle used to stitch you up, gauze to clean you up, gauze to bandage you, tape, ER bed laundry, facility charge, ER room charge, and so on . . . you think all that's included in the $1500, but the $1500 is only to "stitch you up" which, you later find out, means "the service of putting stitches in your arm, and does not include the stitches themselves, the needle used to do the stitching or any of the attendant sundries that one might think would be included in the quoted price". It's like shopping for mattresses, what with all the different names for the same damned product, and all of the supposedly different manufacturers which are really the same damned manufacturer . . . only you don't really have the choice not to buy health care. They've got you, and it's a time sensitive demand for their services.
The weeds is how providers create a false sense of market dislocation so that they can "customize" everything to you, right down to the number of gauze pads they used . . . at exorbitant single use pricing.
Insurers are complicit in this charade because they "helping" the patient with which services are required and "appropriate" pricing for those services. They like the opaqueness because it makes them experts . . . for which they get to charge even more money.
The weeds is what's wrong with American Healthcare. Any normal service provider will quote a price for a complete job, and plan on making money by knowing what the cost of providing the service will be - whether by actuarial tables or experience or whatever - and work at providing competent services while keeping the costs of providing the service in line with the quote.
So the first step in fixing health care is to stay out of the weeds . . . that's where the snakes are.
Yup. Agreed on all counts.That's right, healthcare is nothing but weeds . . . and no one knows what the weeds are when they need medical services. They just know something's wrong and they need some help getting it taken care of.
The weeds is how providers - and insurers - make their money. The weeds is the opaqueness in the health care system.
If you go in for a lacerated arm from a home DIY project, you just want it fixed, and if you ask "how much" you're only impeding getting the arm fixed. If you ask "how much" and they say "$1500 to stitch you up" they don't mention the extra charges for the anesthesia, hypodermic needle for the anesthesia, disinfectant, coagulants, stitch material, the needle used to stitch you up, gauze to clean you up, gauze to bandage you, tape, ER bed laundry, facility charge, ER room charge, and so on . . . you think all that's included in the $1500, but the $1500 is only to "stitch you up" which, you later find out, means "the service of putting stitches in your arm, and does not include the stitches themselves, the needle used to do the stitching or any of the attendant sundries that one might think would be included in the quoted price". It's like shopping for mattresses, what with all the different names for the same damned product, and all of the supposedly different manufacturers which are really the same damned manufacturer . . . only you don't really have the choice not to buy health care. They've got you, and it's a time sensitive demand for their services.
The weeds is how providers create a false sense of market dislocation so that they can "customize" everything to you, right down to the number of gauze pads they used . . . at exorbitant single use pricing.
Insurers are complicit in this charade because they "helping" the patient with which services are required and "appropriate" pricing for those services. They like the opaqueness because it makes them experts . . . for which they get to charge even more money.
The weeds is what's wrong with American Healthcare. Any normal service provider will quote a price for a complete job, and plan on making money by knowing what the cost of providing the service will be - whether by actuarial tables or experience or whatever - and work at providing competent services while keeping the costs of providing the service in line with the quote.
So the first step in fixing health care is to stay out of the weeds . . . that's where the snakes are.
That's right, healthcare is nothing but weeds . . . and no one knows what the weeds are when they need medical services. They just know something's wrong and they need some help getting it taken care of.
The weeds is how providers - and insurers - make their money. The weeds is the opaqueness in the health care system.
If you go in for a lacerated arm from a home DIY project, you just want it fixed, and if you ask "how much" you're only impeding getting the arm fixed. If you ask "how much" and they say "$1500 to stitch you up" they don't mention the extra charges for the anesthesia, hypodermic needle for the anesthesia, disinfectant, coagulants, stitch material, the needle used to stitch you up, gauze to clean you up, gauze to bandage you, tape, ER bed laundry, facility charge, ER room charge, and so on . . . you think all that's included in the $1500, but the $1500 is only to "stitch you up" which, you later find out, means "the service of putting stitches in your arm, and does not include the stitches themselves, the needle used to do the stitching or any of the attendant sundries that one might think would be included in the quoted price". It's like shopping for mattresses, what with all the different names for the same damned product, and all of the supposedly different manufacturers which are really the same damned manufacturer . . . only you don't really have the choice not to buy health care. They've got you, and it's a time sensitive demand for their services.
The weeds is how providers create a false sense of market dislocation so that they can "customize" everything to you, right down to the number of gauze pads they used . . . at exorbitant single use pricing.
Insurers are complicit in this charade because they "helping" the patient with which services are required and "appropriate" pricing for those services. They like the opaqueness because it makes them experts . . . for which they get to charge even more money.
The weeds is what's wrong with American Healthcare. Any normal service provider will quote a price for a complete job, and plan on making money by knowing what the cost of providing the service will be - whether by actuarial tables or experience or whatever - and work at providing competent services while keeping the costs of providing the service in line with the quote.
So the first step in fixing health care is to stay out of the weeds . . . that's where the snakes are.
The last person a hospital wants to see is an injured attorney.
Painting shutters, replacing the garage door opener or cleaning the gutters?
Cutting a tree down, when I was 21 . . . and the cut was on my leg . . . ahh the memories.The last person a hospital wants to see is an injured attorney.
Painting shutters, replacing the garage door opener or cleaning the gutters?
https://www.google.com/amp/s/www.po...2/bernie-sanders-nevada-culinary-union-114687 Speaking of unions, more good work by the Bernie Bros.
Cutting a tree down, when I was 21 . . . and the cut was on my leg . . . ahh the memories.
A little dirt rubbed on it. A little duct tape. Presto. No $1,500.
Checks and money orders accepted.
Never went in . . . still have the scar. Hydrogen peroxide and a band-aid . . .A little dirt rubbed on it. A little duct tape. Presto. No $1,500.
Checks and money orders accepted.
. . . I made up the story in my post . . . believable, though, wasn't it?

I expected Marvin to pull out that argument. That's precisely the argument Big Pharma and their ilk peddle to keep people under their thumb. Basically you're arguing in favor of living a lousy, unhealthy life, then finishing with an even worse one. Makes no sense.Staying healthy longer can mean more of us facing Alzheimer's which I see as becoming a more prevalent and expensive problem in the years ahead.
So you save money in the short run by staying healthy only to run up huge costs in the final years of a long life.
Seems like we cannot win.
No need for Alzheimer's and such to run up costs. There's hospice, living wills, and other solutions to prevent burdening your loved ones. Everyone's free to choose, but living a full, healthy life before losing your marbles ought to be plenty for any normal person, then go out with dignity.
You reminded me of another issue I rarely see mentioned. The US has space. Per capita, lots of space. Compared to Europe and most countries, that's great, except for public transportation, postal services and...the provision of health care. That alone makes it difficult to compare universal health care programs of those densely populated countries with the US.Everyone is right, Healthcare is a giant cluster ****.
I always come back to believing in the checks and balances between the public and private sector in general as that to me is a good starting point.
When you look at other models globally they tend to work together (I think only two countries are 100% single payer).
More importantly I can point to other industries that have a competitive private and public balance like the post office, our school system or security.
Back in the day the fastest choice you had was two day service from the post office. Then a private company called fed ex said it will cost you more but we will deliver it if you absolutely, positively need to get it there overnight. That put pressure on the USPS.
That relationship has always been the public sector kept things affordable while the private sector made sure the government program kept up and offered a competitive product.
When you take one of those two away, in general the private sector gets greedy or the public sector gets complacent.
So in my head at a 50,000 feet level I think we need both to work together and compete against each other....which again is why I like Pete's vision of health care reform.
You reminded me of another issue I rarely see mentioned. The US has space. Per capita, lots of space. Compared to Europe and most countries, that's great, except for public transportation, postal services and...the provision of health care. That alone makes it difficult to compare universal health care programs of those densely populated countries with the US.
Did you know that the US has a higher population density than Sweden, Norway, Finland, and Canada? All have some form of universal health care.
When I posted that I thought about comparable countries: Canada, Russia, maybe Australia. The Scandinavian countries are similar to Canada geographically but much smaller. Per capita was shorthand for describing sparsely populated areas where healthcare services might be far away.Did you know that the US has a higher population density than Sweden, Norway, Finland, and Canada? All have some form of universal health care.
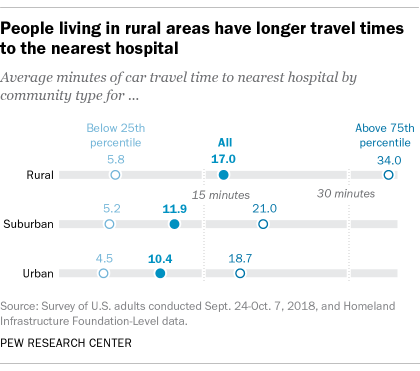
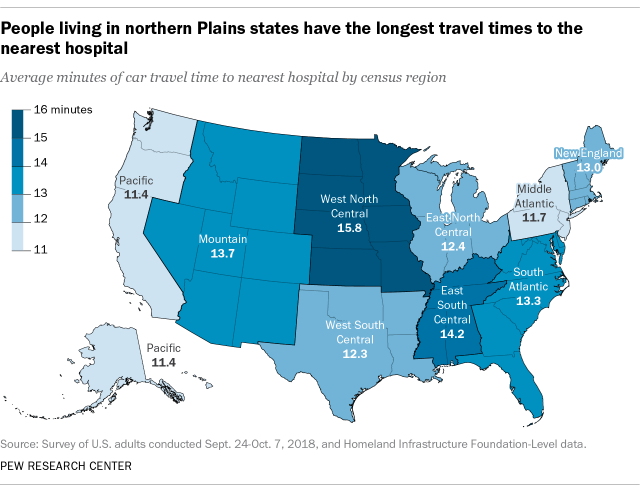
The key here is the 25% who live 34 minutes or more from the nearest hospital. That number is probably worse for certain regions:
I tried to find such data about any Scandinavian country but failed. They do have their sparse regions of course:
That same Pew article links to the NYT that 64 rural hospitals closed between 2013 and 2017. That's a worrisome trend, independent of our health care system.
~~~~
Another factor in an abrupt change of systems is the socio-cultural aspect. I lived in Slovenia for a couple of decades, similar to Zizkov in the Chech Republic. I experienced much the same as he decribes. He omits a number of things that bear considering.Off the top of my head, for example:
1. The current Slovenian health care system pretty much dates back to the end of WW2. The medical infrastructure is thus well established and geographically positioned for an optimal system. It's a lot easier to build a house from scratch than seriously renovate an old one. Ask any builder.
2. Slovenians are very "obedient" and well trained in the system. They are enculturated into the health care system. Getting a society to adopt a new system is probably even harder than renovating an old house.
3. In Slovenia, I got great service. D'oh! I'm American and treated as a guest. I knew that and full well took advantage of it. I bet ZIzkov does too, or at least the medical staff does, whether he's oblivious to it or not. Point being, there are any number of stories about bad service in Slovenia, despite their doctors having received top training in the US and Europe. There are good doctors and bad, like anywhere.
Adopting a MFA in the US is a radical change and in my view, the biggest problem is the doctors. Our doctors like their standard of living. Take that away and our best will pick different professions.
I expected Marvin to pull out that argument. That's precisely the argument Big Pharma and their ilk peddle to keep people under their thumb. Basically you're arguing in favor of living a lousy, unhealthy life, then finishing with an even worse one. Makes no sense.
No need for Alzheimer's and such to run up costs. There's hospice, living wills, and other solutions to prevent burdening your loved ones. Everyone's free to choose, but living a full, healthy life before losing your marbles ought to be plenty for any normal person, then go out with dignity.
IUW, completely agree with everything you write.
Nevertheless, my concern is that many families and the nation as a whole simply are not prepared to dealing with what is already the most expensive disease in America and is projected to grow worse. I call your attention to this article entitled Alzheimer's; The most Expensive Disease in America which in part states...
The overall costs of healthcare are astounding, but the financial burden of an Alzheimer’s diagnosis affects families, too. How much does an Alzheimer’s diagnosis cost individually? According to the Association, Alzheimer’s costs $341,000 on average for the health needs of someone from diagnosis to death. Families pay 70 percent of this out of pocket.
Two comments.IUW, completely agree with everything you write.
Nevertheless, my concern is that many families and the nation as a whole simply are not prepared to dealing with what is already the most expensive disease in America and is projected to grow worse. I call your attention to this article entitled Alzheimer's; The most Expensive Disease in America which in part states...
The overall costs of healthcare are astounding, but the financial burden of an Alzheimer’s diagnosis affects families, too. How much does an Alzheimer’s diagnosis cost individually? According to the Association, Alzheimer’s costs $341,000 on average for the health needs of someone from diagnosis to death. Families pay 70 percent of this out of pocket.
1. The world at large tends to take such illnesses as Alzheimer's inevitable (longevity etc). I would argue they're largely a product of unhealthy lifestyles, diets, and Big Pharma mindset (solve your problems with a pill while ignoring the ever-worsening side effects). A vicious cycle of making unhealthy people live longer.
2. Your article doesn't elaborate on the costs. The system is set up to accrue costs. Alzheimer's and such are big-time money earners for the insidious MBA-driven healthcare system and Big Pharma. TV is dominated by ads intended to hook young people on medications ("Is your neighbor a pain in the butt? Tell your doctor you need some PITA lozenges. Do not take if you are allergic to PITA lozenges, had periods of insomnia, depression, suicidal thoughts, nagging cough, nagging wife...").
In other words, we have an epidemic socio-cultural problem that has nothing to do with MFA.
Link?Two comments.
1. The world at large tends to take such illnesses as Alzheimer's inevitable (longevity etc). I would argue they're largely a product of unhealthy lifestyles, diets, and Big Pharma mindset (solve your problems with a pill while ignoring the ever-worsening side effects). A vicious cycle of making unhealthy people live longer.
2. Your article doesn't elaborate on the costs. The system is set up to accrue costs. Alzheimer's and such are big-time money earners for the insidious MBA-driven healthcare system and Big Pharma. TV is dominated by ads intended to hook young people on medications ("Is your neighbor a pain in the butt? Tell your doctor you need some PITA lozenges. Do not take if you are allergic to PITA lozenges, had periods of insomnia, depression, suicidal thoughts, nagging cough, nagging wife...").
In other words, we have an epidemic socio-cultural problem that has nothing to do with MFA.
To what? My opinion? I've never found a reliable link to my mind...Link?
Dope creek gave a like, Chuckle Chuckle!To what? My opinion? I've never found a reliable link to my mind...
If Vegas puts your weight plus Turtle Dump's at 750 lbs, I'll take the over.Dope creek gave a like, Chuckle Chuckle!
Aww, it's cute that you're responding to Lucifer . . . .If Vegas puts your weight plus Turtle Dump's at 750 lbs, I'll take the over.
Two comments.
1. The world at large tends to take such illnesses as Alzheimer's inevitable (longevity etc). I would argue they're largely a product of unhealthy lifestyles, diets, and Big Pharma mindset (solve your problems with a pill while ignoring the ever-worsening side effects). A vicious cycle of making unhealthy people live longer.
2. Your article doesn't elaborate on the costs. The system is set up to accrue costs. Alzheimer's and such are big-time money earners for the insidious MBA-driven healthcare system and Big Pharma. TV is dominated by ads intended to hook young people on medications ("Is your neighbor a pain in the butt? Tell your doctor you need some PITA lozenges. Do not take if you are allergic to PITA lozenges, had periods of insomnia, depression, suicidal thoughts, nagging cough, nagging wife...").
In other words, we have an epidemic socio-cultural problem that has nothing to do with MFA.
IUW, in addition to multiple factors, such as genetics, lifestyle, age, and environment., i will add Big Pharma as a possible cause of Alzheimer's. Quite frankly, I had not considered Big Pharma medications as contributing to Alzheimer.s as a side effect until reading your post.
Someday researchers may confirm this along with pinning down causes and cures more precisely.
Or the opposite. God forbid you run up huge financial costs when you're young. Then you can be totally screwed later in life. Many of these policies have a lifetime cap on what they pay out and if you exhaust it early you're toast. I know a guy who was taking heavy doses of prednisone for years. For some that can turn your tissue into kleenex. He had an endoscopy done and it punctured a hole in his esophagus. He was in the hospital for almost 9 months. The hospital/doctors exceeded his health insurance lifetime cap. Now he's basically uninsurable.
Lifetime caps and insurance price ratings based upon pre- existing conditions are both outlawed via the ACA..... so not sure what you are talking about. What you described used to be completely accurate, but hasn't been for 6 years.
I knew that on pre-existing but didn't on caps. So I'm six years behind. Par for the course for me. Thanks.Lifetime caps and insurance price ratings based upon pre- existing conditions are both outlawed via the ACA..... so not sure what you are talking about. What you described used to be completely accurate, but hasn't been for 6 years.
Two comments.
1. The world at large tends to take such illnesses as Alzheimer's inevitable (longevity etc). I would argue they're largely a product of unhealthy lifestyles, diets, and Big Pharma mindset (solve your problems with a pill while ignoring the ever-worsening side effects). A vicious cycle of making unhealthy people live longer.
2. Your article doesn't elaborate on the costs. The system is set up to accrue costs. Alzheimer's and such are big-time money earners for the insidious MBA-driven healthcare system and Big Pharma. TV is dominated by ads intended to hook young people on medications ("Is your neighbor a pain in the butt? Tell your doctor you need some PITA lozenges. Do not take if you are allergic to PITA lozenges, had periods of insomnia, depression, suicidal thoughts, nagging cough, nagging wife...").
In other words, we have an epidemic socio-cultural problem that has nothing to do with MFA.
So, what would you advocate for a family whose loved one currently faces an Alzheimer's diagnosis?
So, what would you advocate for a family whose loved one currently faces an Alzheimer's diagnosis?
Patience, support, and a whole lot of subsidized help. That's a special kind of love, to take care of someone whose memory is going or gone.So, what would you advocate for a family whose loved one currently faces an Alzheimer's diagnosis?
I have a buddy - a retired pediatrician - whose wife is slipping into memory loss. It's happening faster now, but a year or so ago he told me some really cute, but heartbreaking, stories.
Once while they were still living together - she's in a Memory Care unit now, which is on the same campus, but separate from where he's living - he helped prepare dinner with her. They chatted and got on well. After dinner they went for a walk around the grounds of their retirement center, and she confided in him that she really kinda liked the guy she had dinner with . . .
. . . what do you say to that?
Anyway, the cost of memory care is causing him to go broke, financially. He's in his 80s . . . what do you do?
He often quotes Philip Roth: Old age isn't a battle, it's a massacre.
Last edited:
Who me? I'm no expert but I did take care of my mom for her last six years. I treasured every moment, so that's one recommendation. I also spent a lot of time with my dad in is latter days. In dealing with my own future grief, which overtook me in advance occasionally, I had a realization that he didn't want to spend time with me being sad. From that moment on, I had fun with him. And he did too.So, what would you advocate for a family whose loved one currently faces an Alzheimer's diagnosis?
Both my parents wrote living wills well in advance of their slippage.
Real conversations are useful, I think, especially letting the ill person talk, talk, talk about what they're going through, so they're not alone. A lot of senior people seem to think they're a burden and don't want to put their burden on others, especially their family. That includes not talking about it and that may be what they need most.
~~~~
Mainly, my thrust is for a paradigm shift, focusing on the future. That shift won't help today's seniors.
Mom's was: Getting old's not for sissies.Patience, support, and a whole lot of subsidized help. That's a special kind of love, to take care of someone whose memory is going or gone.
I have a buddy - a retired pediatrician - whose wife is slipping into memory loss. It's happening faster now, but a year or so ago he told me some really cute, but heartbreaking, stories.
Once while they were still living together - she's in a Memory Care unit now, which is on the same campus, but separate from where he's living - he helped prepare dinner with her. They chatted and got on well. After dinner they went for a walk around the grounds of their retirement center, and she confided in him that she really kinda liked the guy she had dinner with . . .
. . . what do you say to that?
Anyway, the cost of memory care is causing him to go broke, financially. He's in his 80s . . . what do you do?
He often quotes Philip Roth: Old age isn't a battle, it's a massacre.
My children's cousin took her grandmother to a pristine pond with a quaint church at the far end. Granny said, "Oh what a beautiful church. Let's walk over there." They walked around to the church, then continued back around to the beginning. Granny looked across the pond and said, "Oh what a beautiful church. Let's walk over there."
When Dad, 88, was at Bell Trace, in rehab (he never made it out), shortly after he got there an old geezer of about 98 wheeled in to Dad's room and started trying to sell Dad life insurance...
Same guy's wife, 96, was also there in a wheel chair. Once I saw him pushing her along from behind, two-chair tandem, and she was reading the names on each door, Sam Jones, Jane Wester... Then he goes, "Where're we going?" She responds, "I dunno. You're driving."
One time we're sitting in the dining room. Dad looks across and sees a volunteer whose body shape is tall, very large, and shaped like a top, symmetrically conical above and below. He unabashedly exclaims, "Wow! She's plump!"
Today's NYT has an article on this:We pay whatever the hell the bill says, and we don't know what the bill will say until we receive it (mainly talking healthcare). What other market can operate like this....would you get a car not knowing the cost, or put groceries in your cart without any clue of what the price tag was? The conversation needs to be about correcting the cost issue and making it transparent
Surprise bills are just the latest weapons in a decades-long war between the players in the health care industry over who gets to keep the fortunes generated each year from patient illness — $3.6 trillion in 2018.
Here’s how they came to be:
Forty years ago, when many insurers were nonprofit entities, and being a doctor wasn’t seen as a particularly good entree into the 1 percent, billed rates were far lower than they are today, and insurers mostly just paid them. Premiums were low or paid by an employer. Patients paid little or nothing in co-payments or deductibles.
That’s when a more entrepreneurial streak kicked in. Think about the opportunities: If someone is paying you whatever you ask, why not ask for more?
Commercial insurers as well as Blue Cross Blue Shield Plans, some of which had converted to for-profit status by 2000, began to push back on escalating fees from providers, demanding discounts.
Hospitals and doctors argued about who got to keep different streams of revenue they were paid. Doctors began to form their own companies and built their own outpatient surgery centers to capture payments for themselves.
So today your hospital and doctor and insurer — all claiming to coordinate care for your health — are often in a three-way competition for your money.
As the battle for revenue has heated up, each side has added new weapons to capture more: Hospitals added facility fees and infusion charges. Insurers levied ever-rising copayments and deductibles. Most important they limited the networks of providers to those that would accept the rates they were willing to pay.
Surprise bills are the latest tactic: When providers decided that an insurer’s contracted payment offerings were too meager, they stopped participating in the insurer’s network; either they walked away or the insurer left them out. In some cases, physicians decided not to participate in any networks at all. That way, they could charge whatever they wanted when they got involved in patient care and bill the patient directly. For their part, insurers didn’t really care if those practitioners demanding more money left.
And, for a time, all sides were basically fine with this arrangement.
But as the scope and the scale of surprise bills has grown in the past five years, more people have experienced these costly, unpleasant surprises. With accumulating bad publicity, they have became impossible to ignore. It was hard to defend a patient stuck with over $500,000 in surprise bills for 14 weeks of dialysis. Or the $10,000 bill from the out-of-network pediatrician who tends to newborns in intensive care. How about the counties where no ambulance companies participated in insurance, so every ambulance ride costs hundreds, or even thousands of dollars?
These practices are an obvious outrage. But no one in the health care sector wants to unilaterally make the type of big concessions that would change them. Insurers want to pay a fixed rate. Doctors and hospitals prefer what they call “baseball- style arbitration,” where a reasonable charge is determined by mediation. Both camps have lined up sympathetic politicians for their point of view.
So, nothing has changed at the federal level, even though it’s hard to imagine another issue for which there is such widespread consensus. Two-thirds of Americans say they are worried about being able to afford an unexpected medical bill — more than any other household expense. Nearly eight in 10 Americans say they want federal legislation to protect patients against surprise bills.
States are passing their own surprise billing laws, though they lack power since much of insurance is regulated at a national level.
Now, members of Congress have yet another chance to tackle this obvious injustice. Will they listen to hospitals, doctors, insurers? Or, in this election year, will they finally heed their voter-patients?
CBS ran a story on Coffeyville, KS. A lawyer convinced a judge to require people with medical debt to report to court and swear they cannot afford to pay. If they miss twice, contempt of court. Here is the part that should anger people, the lawyer makes profit off of this. https://people.com/health/dad-jaile...s-leukemia-treatments-and-wifes-seizures/amp/
No idea what Kansas law is but this is really strange. I presume the case is on a state court, civil, bulk collections docket. If that's the case I have no idea why it's contempt and a warrant instead of just a default and then a default jdgmt. Sounds like a nutty, rogue judge making his own rules of procedure.CBS ran a story on Coffeyville, KS. A lawyer convinced a judge to require people with medical debt to report to court and swear they cannot afford to pay. If they miss twice, contempt of court. Here is the part that should anger people, the lawyer makes profit off of this. https://people.com/health/dad-jaile...s-leukemia-treatments-and-wifes-seizures/amp/
Last edited:
The tax considerations were secondary. Our current system is an unintended consequence of post WWII wage controls. It started under Truman. Wage controls were in place, so the unions couldn't negotiate for more pay and had to look for other ways their members could participate in the post-war boom. Health insurance was what they went for, and employee provided insurance soon became commonplace. As wage controls weren't the case in other developed countries, they took different approaches that put a much greater emphasis on government participation.Unions traded wages for better benefits..... this was actually a wise choice as benefits aren't taxable, where wages obviously are.
The tax considerations were secondary. Our current system is an unintended consequence of post WWII wage controls. It started under Truman. Wage controls were in place, so the unions couldn't negotiate for more pay and had to look for other ways their members could participate in the post-war boom. Health insurance was what they went for, and employee provided insurance soon became commonplace. As wage controls weren't the case in other developed countries, they took different approaches that put a much greater emphasis on government participation.
Yep. I always explain this to people when they start lamenting our screwy HC system. Almost nobody knows this (or remembers it).
We got here by accident. Nobody would ever intentionally create such a messed up system.
But the point about unions.... they continued to do the economical rationale thing under the system we all operate under. For the last several decades, it's filtered down to everyone..... trading lower wages for ever more expensive HC coverage. Total comp has increased.... but nobody sees it. Unless you own/ manage a business providing insurance to employees.... then you know how large a burden of the total comp package it is.
Similar threads
- Replies
- 77
- Views
- 3K
- Replies
- 125
- Views
- 7K
- Replies
- 164
- Views
- 11K
ADVERTISEMENT
ADVERTISEMENT