What’s more there are myriad problems with broad categories and definitions. What does isolate mean. If you deem vulnerable those with pre-existing or over a certain age what if they don’t wish to be isolated (con rights etc). I am a broken record I know. It’s just the current course isn’t any solution. It’s kicking the can in hopes of a vaccine that may never arrive. It’s hope against hope, while the attendant/collateral damage grows exponentiallyNo one can tell ahead of time who is "vulnerable." Even elderly can be asymptomatic.
I-TEAM: Asymptomatic elderly patients identified in two local nursing homes
An outbreak at a local nursing home has stunned families and even healthcare workers. How could more 70 patients and nearly 20 employees test positive for COVID-19 without warning?www.wrdw.com

Colleges
- AAC
- ACC
- Big 12
- Big East
- Big Ten
- Pac-12
- SEC
- Atlantic 10
- Conference USA
- Independents
- Junior College
- Mountain West
- Sun Belt
- MAC
- More
- Navy
- UAB
- Tulsa
- UTSA
- Charlotte
- Florida Atlantic
- Temple
- Rice
- East Carolina
- USF
- SMU
- North Texas
- Tulane
- Memphis
- Miami
- Louisville
- Virginia
- Syracuse
- Wake Forest
- Duke
- Boston College
- Virginia Tech
- Georgia Tech
- Pittsburgh
- North Carolina
- North Carolina State
- Clemson
- Florida State
- Cincinnati
- BYU
- Houston
- Iowa State
- Kansas State
- Kansas
- Texas
- Oklahoma State
- TCU
- Texas Tech
- Baylor
- Oklahoma
- UCF
- West Virginia
- Wisconsin
- Penn State
- Ohio State
- Purdue
- Minnesota
- Iowa
- Nebraska
- Illinois
- Indiana
- Rutgers
- Michigan State
- Maryland
- Michigan
- Northwestern
- Arizona State
- Oregon State
- UCLA
- Colorado
- Stanford
- Oregon
- Arizona
- California
- Washington
- USC
- Utah
- Washington State
- Texas A&M
- Auburn
- Mississippi State
- Kentucky
- South Carolina
- Arkansas
- Florida
- Missouri
- Ole Miss
- Alabama
- LSU
- Georgia
- Vanderbilt
- Tennessee
- Louisiana Tech
- New Mexico State
- Middle Tennessee
- Western Kentucky
- UTEP
- Florida International University
High School
- West
- Midwest
- Northeast
- Southeast
- Other
- Alaska
- Arizona
- California
- Colorado
- Nevada
- New Mexico
- Northern California
- Oregon
- Southern California Preps
- Washington
- Edgy Tim
- Indiana
- Kansas
- Nebraska
- Iowa
- Michigan
- Minnesota
- Missouri
- Oklahoma Varsity
- Texas Basketball
- Texas
- Wisconsin
- Delaware
- Maryland
- New Jersey Basketball
- New Jersey
- New York City Basketball
- Ohio
- Pennsylvania
- Greater Cincinnati
- Virginia
- West Virginia Preps
ADVERTISEMENT
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Long Covid
- Thread starter sglowrider
- Start date
Agree. It will be a while before approval and even longer to get it to a significant part of the population.
Yep. And that presupposes we get one that’s viable
A reasonable form of pessimism at this point.I’m losing faith in a vaccine anytime soon....
Goat that mischaracterizes what he’s arguing: isolate the vulnerable and let it run through the the 99.8% plus that won’t die from it. I don’t know if that is prudent or not. It may be our only option if a vaccine isn’t in the offing. What’s kicking the can is the current mantra of new cases, new cases, new cases, followed by lockdowns with little regard to the staggering consequences of lockdowns from poverty (insidious health issues), educational setbacks, lost livelihoods, blah blah blah.
goat is quite aware that he's mischaracterizing what i said.
that's what he does when he has nothing else, despite how immoral.
and what you mischaracterized as what i meant, also isn't so.
there is nothing unclear about the position i've pushed.
let it run through the 60% who relatively aren't at risk.
and the additional maybe 10% who are at risk, but have already voluntarily chosen and taken that route already, and i couldn't stop them if i wanted to.
that very soon gives you a large herd immune base to keep the economy going, and allows those not at risk and those "at risk but don't care", to return to normal life, and a normal economy.
while doing so, use part of the trillions saved by going back to normal life for that 60% plus percent who do 90% of the discretionary spending, to finance those who are are risk, and wish to take safe haven, to financially and logistically safely do so in the mean time..
meanwhile, continue vaccine and treatment research full steam ahead.
society is already taking this path anyway, like it or not.
except more slowly, and without saving the economy, and without financially and logistically enabling safe haven for those who are at risk.
i'm merely acknowledging the reality of what's already happening and can't be stopped, accelerating it for the "not at risk" and "don't care" universes, and totally freeing them and the economy in the process.
meanwhile, i'm financially and logistically allowing safe haven for those who do need and want it. (and doing so at a fraction of the current boondoggle cost).
and i'm doing so, because hoping everyone will distance and mask for another yr plus, when obviously they won't, while not lending any safe haven to those who need and want it, while destroying the economy and the currency in the process, which is precisely what is currently happening despite what everyone hopes should be happening, which is a total and complete failure of epic proportion on every level, with little to zero hope of anything improving indefinitely, either health or economy wise.
and again, i totally welcome any better ideas.
wishing isn't a better idea.
what's currently happening isn't a better idea.
Last edited:
Goat that mischaracterizes what he’s arguing: isolate the vulnerable and let it run through the the 99.8% plus that won’t die from it. I don’t know if that is prudent or not. It may be our only option if a vaccine isn’t in the offing. What’s kicking the can is the current mantra of new cases, new cases, new cases, followed by lockdowns with little regard to the staggering consequences of lockdowns from poverty (insidious health issues), educational setbacks, lost livelihoods, blah blah blah. The rub is do we have any evidence that herd immunity is achievable with this particular virus?
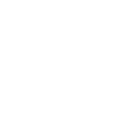
We had this debate back in the spring. Yes we could take this track. We'd end up with probably about 2m excess deaths (in the US) over the next year or so. Worldwide some 25-50m people died in 1918-19..... reasonable to think that would be the case again, early mortality rates of covid seem to be in the general range of the 1918 flu.
Supportive care obviously better today than 100 years ago, but not exponentially. It's still a novel virus, with no existing immunity.
The history of 1918 is the best touch point we have to work off.
Spanish flu - Wikipedia
But it would "work".... in that it would be fairly quickly over with, if we just let half the world's population get infected. We'd also likely bust our health care systems during this time. I highly doubt there are too many seniors that want to roll the dice with such a strategy.
It's a fkn mess.... I'm quite concerned about this winter. The 2nd wave of the 1918 virus was much more powerful. Maybe we'll get lucky and it'll go the opposite direction this time.

I’m losing faith in a vaccine anytime soon....
Many are very optimistic about RNA vaccines. Covid-19 is the first important use. Trials so far are very encouraging.
Good article written before the Covid pandemic.
I’m losing faith in a vaccine anytime soon....
Q1 next year. Not expected to be 100% for all ages and demographics. But healthcare workers will be first then if safe the vulnerables like elderly.
Folks like me and you probably by 2022 unless they run out of materials. Then there is the issue of price too.
The vulnerable can't be isolated. We let it spread, it will get to everyone eventually.
Right, we know the vulnerable cannot be isolated because it is still getting into nursing homes. We know that the spread right now is mostly from small gatherings. People are choosing not to wall themselves into homes. They are choosing not to avoid all human contact. In one month, roughly 40,000 IU students will head home for Thanksgiving. Does anyone really think their parents are going to lock them out? Their grandparents?
If you focus on any one vaccine, statistically speaking, it is likely to fail to meet endpoints in clinical trials. Meeting endpoints in a clinical trial is a high bar. Safety, efficacy, dose dependence, all with clear statistics.
But we are taking so many shots on goal with so many different strategies, statistically speaking, it is in fact very likely that a few of them will meet endpoints in clinical trials.
I am guessing limted use approval of at least one by January, more extensive approval by March, multiple options by May, 50% USA population coverage for those who want it by this time next year. Not blazing fast, but OK. We need to make more people want it.
But we are taking so many shots on goal with so many different strategies, statistically speaking, it is in fact very likely that a few of them will meet endpoints in clinical trials.
I am guessing limted use approval of at least one by January, more extensive approval by March, multiple options by May, 50% USA population coverage for those who want it by this time next year. Not blazing fast, but OK. We need to make more people want it.
Right, we know the vulnerable cannot be isolated because it is still getting into nursing homes. We know that the spread right now is mostly from small gatherings. People are choosing not to wall themselves into homes. They are choosing not to avoid all human contact. In one month, roughly 40,000 IU students will head home for Thanksgiving. Does anyone really think their parents are going to lock them out? Their grandparents?
nursing homes by definition are not an isolated environment. Duh!
that said, are grandparents doing Thanksgiving with their kids and college attending grandchildren in your household?
If you focus on any one vaccine, statistically speaking, it is likely to fail to meet endpoints in clinical trials. Meeting endpoints in a clinical trial is a high bar. Safety, efficacy, dose dependence, all with clear statistics.
But we are taking so many shots on goal with so many different strategies, statistically speaking, it is in fact very likely that a few of them will meet endpoints in clinical trials.
I am guessing limted use approval of at least one by January, more extensive approval by March, multiple options by May, 50% USA population coverage for those who want it by this time next year. Not blazing fast, but OK. We need to make more people want it.
I believe they'll likely be massive hesitation within the public to run out and get first in line for a vaccine.
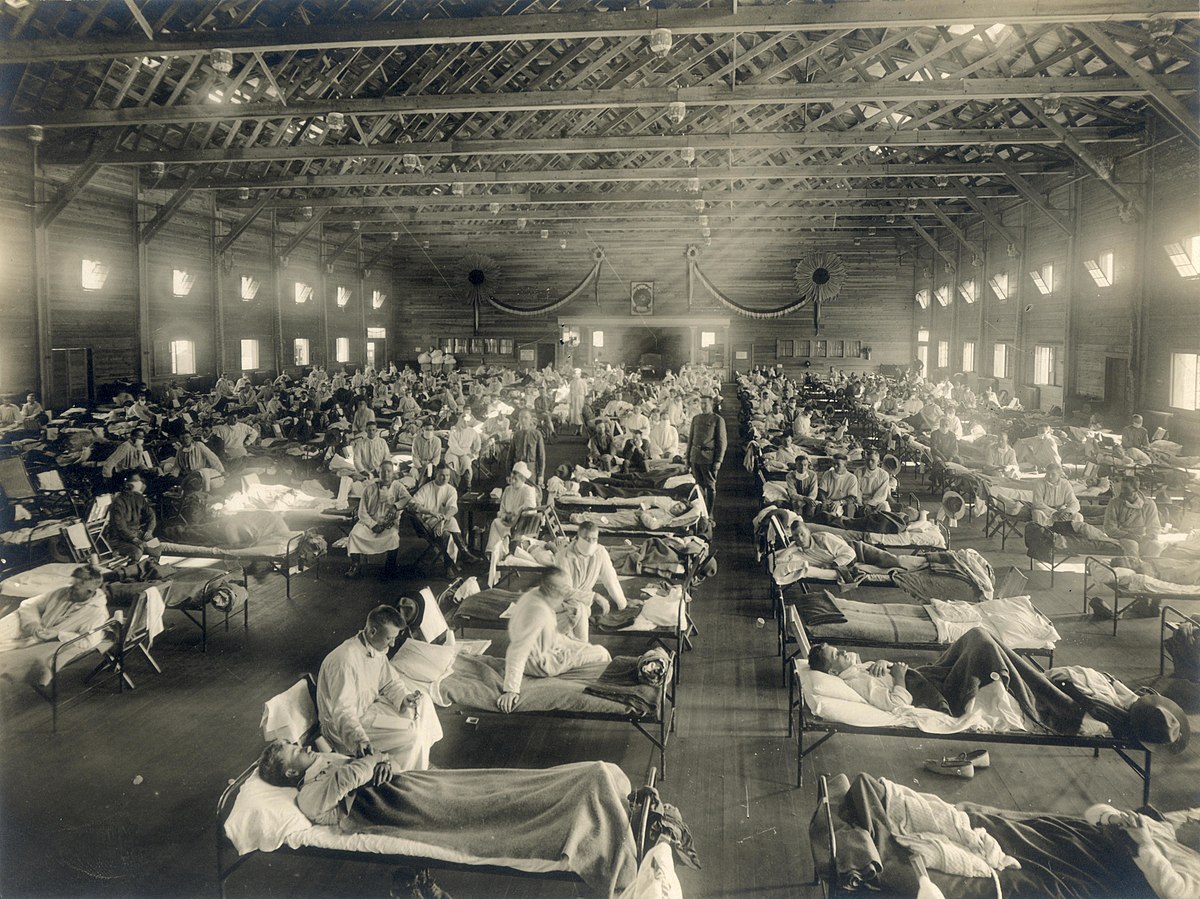
9% of patients were readmitted to the same hospital within 2 months of discharge.
Summary
What is already known about this topic?
Evidence suggests that potential health complications after COVID-19 illness might require ongoing clinical care.
What is added by this report?
After discharge from an initial COVID-19 hospitalization, 9% of patients were readmitted to the same hospital within 2 months of discharge. Multiple readmissions occurred in 1.6% of patients. Risk factors for readmission included age ≥65 years, presence of certain chronic conditions, hospitalization within the 3 months preceding the first COVID-19 hospitalization, and discharge to a skilled nursing facility or with home health care.
What are the implications for public health practice?
Understanding the frequency of and potential reasons for, readmission after a COVID-19 hospitalization can inform clinical practice, discharge disposition decisions, and public health priorities, such as health care resource planning.
Coronavirus disease 2019 (COVID-19) is a complex clinical illness with potential complications that might require ongoing clinical care (1–3).
Summary
What is already known about this topic?
Evidence suggests that potential health complications after COVID-19 illness might require ongoing clinical care.
What is added by this report?
After discharge from an initial COVID-19 hospitalization, 9% of patients were readmitted to the same hospital within 2 months of discharge. Multiple readmissions occurred in 1.6% of patients. Risk factors for readmission included age ≥65 years, presence of certain chronic conditions, hospitalization within the 3 months preceding the first COVID-19 hospitalization, and discharge to a skilled nursing facility or with home health care.
What are the implications for public health practice?
Understanding the frequency of and potential reasons for, readmission after a COVID-19 hospitalization can inform clinical practice, discharge disposition decisions, and public health priorities, such as health care resource planning.
Coronavirus disease 2019 (COVID-19) is a complex clinical illness with potential complications that might require ongoing clinical care (1–3).
Long Covid: doctors find ‘antibody signature’ for patients most at risk
Low levels of certain antibodies found to be more common in those who go on to develop long CovidDoctors have discovered an “antibody signature” that can help identify patients most at risk of developing long Covid, a condition where debilitating symptoms of the disease can persist for many months.
When combined with the patient’s age, details of their Covid symptoms and whether or not they had asthma, the antibody signature allowed doctors to predict whether people had a moderate, high or very high risk of developing long-term illness.
Similar threads
- Replies
- 9
- Views
- 709
- Replies
- 2
- Views
- 157
- Replies
- 6
- Views
- 344
ADVERTISEMENT
ADVERTISEMENT