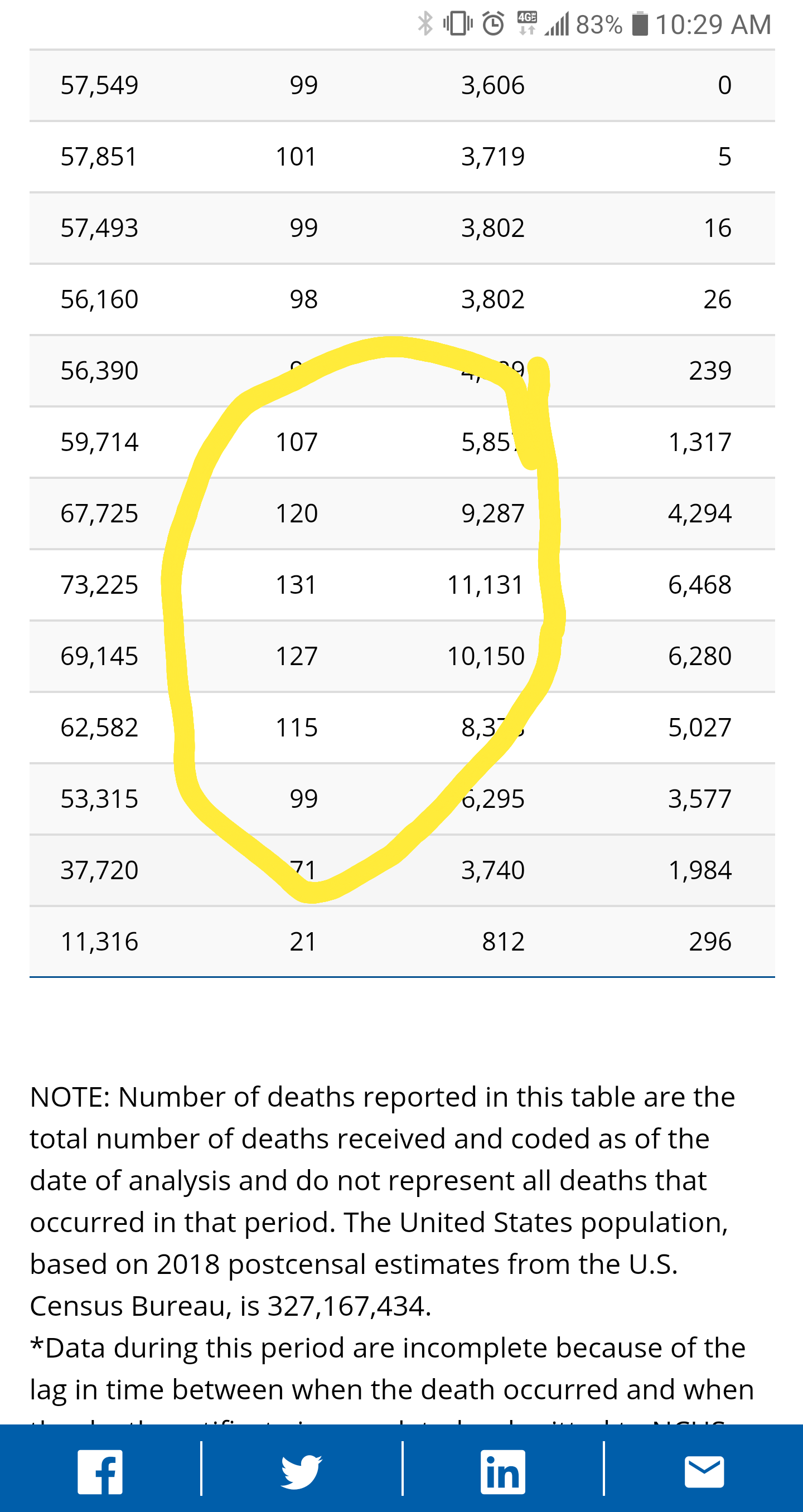
The CDC tracks the number of deaths reported and they differ slightly from media numbers. They provide the criteria for reporting at the bottom of the page.
https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
What I gleaned from the numbers from the CDC and an interpretation of the bubble map on same page is we have had 67,008 deaths attributed to COVID-19 in America. Of the 67,008, 32,998 come from New York and New Jersey (49%).
I was looking for Nursing Home statistics and was surprised to find that Nursing Homes are not required to report according to AARP. The numbers I found were provided by AARP and they claim More than 16,000 deaths in Nursing Homes across the nation. Let’s assume New York and New Jersey numbers hold to their percentage of overall deaths and account for 49% of Nursing Home Deaths. That would mean 8,160 deaths in Nursing Homes occurred outside of New Jersey and NY.
https://www.aarp.org/caregiving/health/info-2020/coronavirus-nursing-home-cases-deaths.html
What does this mean? Well if you add together NY, NJ, and NH deaths you get 41,158 deaths associated with these three out of 67,008 total deaths. That is a whopping 61.42% of all Corona Virus associated Deaths.
Outside of these three areas, we did really well in limiting the impact of COVID 19. Are you surprised by this? I was. How close does the media drum beat reflect these breakdowns? I don’t think it reflects it at all.
https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm
What I gleaned from the numbers from the CDC and an interpretation of the bubble map on same page is we have had 67,008 deaths attributed to COVID-19 in America. Of the 67,008, 32,998 come from New York and New Jersey (49%).
I was looking for Nursing Home statistics and was surprised to find that Nursing Homes are not required to report according to AARP. The numbers I found were provided by AARP and they claim More than 16,000 deaths in Nursing Homes across the nation. Let’s assume New York and New Jersey numbers hold to their percentage of overall deaths and account for 49% of Nursing Home Deaths. That would mean 8,160 deaths in Nursing Homes occurred outside of New Jersey and NY.
https://www.aarp.org/caregiving/health/info-2020/coronavirus-nursing-home-cases-deaths.html
What does this mean? Well if you add together NY, NJ, and NH deaths you get 41,158 deaths associated with these three out of 67,008 total deaths. That is a whopping 61.42% of all Corona Virus associated Deaths.
Outside of these three areas, we did really well in limiting the impact of COVID 19. Are you surprised by this? I was. How close does the media drum beat reflect these breakdowns? I don’t think it reflects it at all.